AI transformers shed light on the brain’s mysterious astrocytes

Research
Kim Martineau
IBM Research and JDRF continue advancing biomarker research based on IBM’s composite biomarkers discovery toolkit recently released under BiomedSciAI, a repository of tools for accelerated discoveries in health care, and the clinical expertise of our partners to demonstrate how novel biomarkers can address urgent problems in healthcare.
The AI toolkits developed by IBM Research have enabled an international team of researchers to accelerate discoveries of biomarkers for type 1 diabetes (T1D) and their potential applications. IBM’s partnership with JDRF has been the cornerstone of this effort. It has enabled the gathering of highly respected researchers from across the globe, allowing us to merge advanced AI technologies with clinical expertise to achieve these results.
The T1DI Study Group formed in this effort has recently made four more important milestones in this field of research, including our most recent paper in The Lancet Child & Adolescent Health1 which describes how understanding of disease heterogeneity enabled by biomarkers can lead to better screening and early detection of T1D. Such understanding is also important for better design of clinical trials.
Enabled by capabilities in our composite biomarkers discovery toolkit ranging from disease progression modeling, to novel visual analytics of biomarker trajectories, to screening strategy assessment, each of the recent milestones addresses a very different specific need in the field, leading to the following important discoveries:
These milestones address diverse, yet related needs as the team continues both refining potential biomarkers for type 1 diabetes and exploring potential applications of these novel biomarkers to current challenges in this field — particularly with respect to screening for early detection and clinical trial design. These new results, together with our earlier body of work, represent continuing progress on this important topic powered by IBM’s accelerated discovery technology.
“These observations are very important to understand the heterogeneous development of T1D,” Riitta Veijola, principal investigator of the DIPP study in Finland, said. “In particular, the results can be used to design prevention trials for individuals following similar disease pathways.”
“With the 2022 FDA approval of the first drug to delay onset of type 1 diabetes, it’s an exciting time to be working with IBM and the T1DI Study Group on the publication of T1DI analyses to refine our understanding of the heterogeneous progression of the disease prior to onset. The conclusions from the recent publications will spur discussion in the research community and inform the parameters for T1D screening programs being developed worldwide”, says JDRF’s AVP Research, Partnerships, Olivia Lou, Ph.D.
T1D is an autoimmune disease that can strike both children and adults. People diagnosed with T1D confront difficult, life-long disease management issues when adjusting daily insulin therapy, meals, and physical exercise according to their glucose monitoring results. Even with the best management, they are at still at risk of potentially devastating long-term complications such as kidney failure, heart attack, stroke, blindness, and amputation.
While there are treatments for T1D, there is currently no prevention or cure and incidence rates have risen steadily over recent decades. In addition, some cases are only diagnosed when they present with diabetic ketoacidosis (DKA), a life-threatening condition with potentially long-term consequences, making early detection increasingly critical.
Recent data indicates, however, that onset of T1D can be delayed up to two years with immunomodulatory treatment, namely teplizumab, given to very high-risk individuals. This treatment has recently been approved by the FDA for clinical use in the USA. There is also a great deal of ongoing research into other treatments that could potentially delay onset, or possibly even prevent the disease. This means there is new urgency to identifying people who may be at higher risk so that they might be enrolled in appropriate clinical trials.
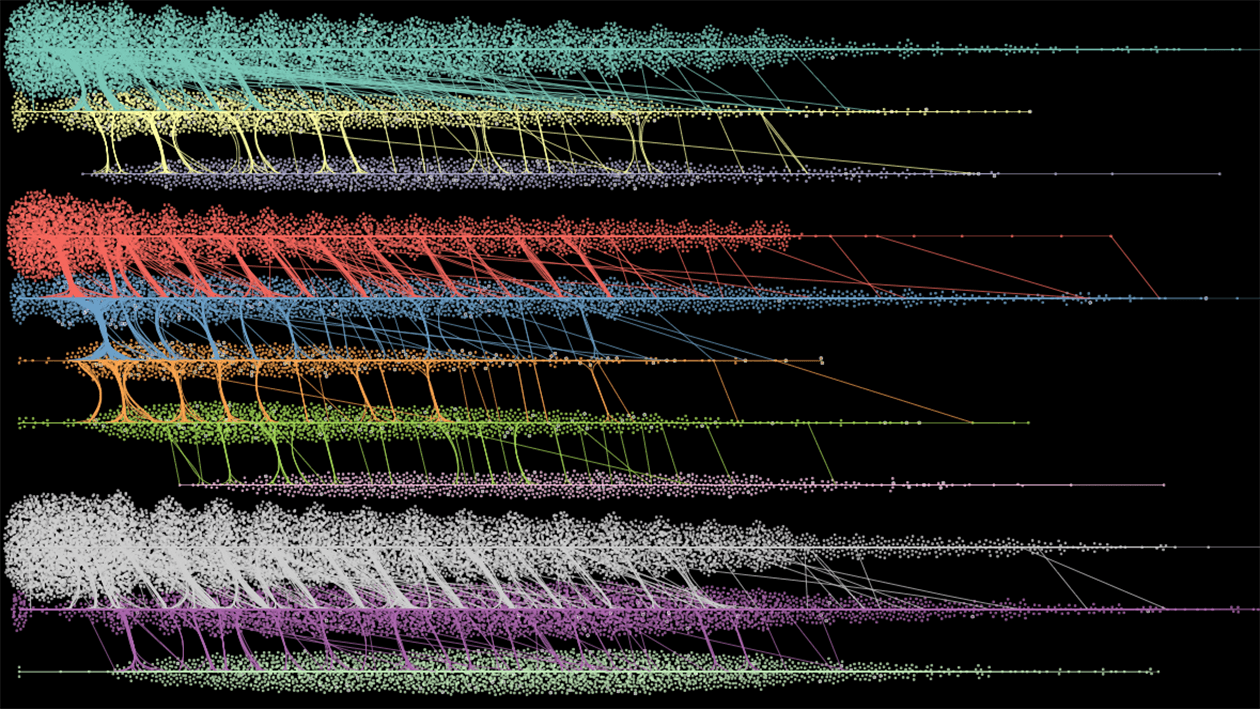
The association between islet autoantibodies and T1D has been known for some time, however, their presence can change over time, so a single negative test does not absolutely mean that a person is completely free of risk of developing T1D. At the same time, individual positive tests do not definitively predict that an individual will develop T1D. Furthermore, these tests cannot accurately predict timing of T1D diagnosis. The complexity of this analysis is apparent in the following image from where we examined the data using our data visualization tools to reveal the impact of islet autoantibody levels on progression to T1D onset across varying patterns of autoantibody level changes up to 20 years of age.3
Our work has helped to refine the predictive value of these biomarkers, helping researchers more reliably differentiate patients at higher levels of risk and rates of progression to onset of clinical disease. Such findings may eventually lead to better monitoring and earlier detection, as well as better design of early intervention trials.
Our most recent papers, one published last August in The Lancet Diabetes & Endocrinology4 and the other published this month in The Lancet Child & Adolescent Health1 describe work we have done to take a logical next step with these developing biomarkers, which is to begin charting a path towards better screening for T1D.
Effective T1D screening is complicated by the fact that disease onset can occur at many different ages so we must determine the appropriate ages at which screening will be most effective. Our latest research does just that. The first of these two papers establishes that screening at just two ages — two and six — is sufficient to detect a large majority of cases that would occur by the age of 15, which may be customizable to the population at risk in different geographic regions.
Since not all cases are diagnosed by age 15 however, our fourth paper further explored the potential impact of screening during adolescence. We found that a single screening test at age 10 can be a strong predictor in this age group. This age group is important in several respects: First, DKA at onset occurs most frequently among toddlers and teenagers,5 which means that adolescents are at particularly high risk of experiencing this serious complication; Second, our research has demonstrated that both the rate and the trajectory of antibody development in this group is different from those with onset during childhood, meaning that a different strategy may be needed for them.
As we think about the importance of these four recent publications together, we can easily see how important advances in biomarker development are. In the case of T1D, they can enable earlier identification of at-risk children and adolescents to avoid negative consequences such as DKA at time of diagnosis, and are critical for better design of clinical trials aimed at developing therapies for preventing or delaying the onset of the disease.
IBM is dedicated to leveraging recent advances in computing technologies to convene and support inter-disciplinary scientific research teams, that will result in the development of improved biomarkers for serious diseases and clinically important findings leading to accelerated discovery of therapeutics. Our work with JDRF on T1D stands out as an example of our approach to enabling accelerated scientific discovery through AI driven technologies and collaboration with communities of discovery, which can lead to important scientific findings and the advancement of medicine.
Ghalwash M, Anand V, Lou O, Martin F, Rewers M, Ziegler AG, Toppari J, Hagopian W, Veijola R. Type 1 Diabetes Intelligence Study Group. Islet Autoantibody Screening in Adolescents at Risk to Predict Type 1 Diabetes Until Young Adulthood: a prospective cohort study. *The Lancet Child & Adolescent Health.*2023, ISSN 2352-4642, ~https://doi.org/10.1016/S2352-4642(22)00350-9 ~ ↩ ↩2 ↩3
Ng K, Anand V, Stavropoulos H, Veijola R, Toppari J, Maziarz M, Lundgren M, Waugh K, Frohnert BI, Martin F, Lou O, Hagopian W, Achenbach P for the T1DI Study Group. Quantifying the utility of islet autoantibody levels in the prediction of type 1 diabetes in children. Diabetologia. 2022. https://doi.org/10.1007/s00125-022-05799-y ↩
Kwon BC, Achenbach P, Anand V, Frohnert BI, Hagopian W, Hu J, Koski E, Lernmark Å, Lou O, Martin F, Ng K, Toppari J, Veijola R; T1DI Study Group. Islet Autoantibody Levels Differentiate Progression Trajectories in Individuals with Presymptomatic Type 1 Diabetes. Diabetes. 2022 Sep 16. doi: 10.2337/db22-0360. Epub ahead of print. PMID: 36112006. ↩ ↩2
Ghalwash M, Dunne JL, Lundgren M, Rewers M, Ziegler AG, Anand V, Toppari J, Veijola R, Hagopian W; Type 1 Diabetes Intelligence Study Group. Two-age islet-autoantibody screening for childhood type 1 diabetes: a prospective cohort study. Lancet Diabetes Endocrinol. 2022 Aug;10(8). doi: 10.1016/S2213-8587(22)00141-3. Epub 2022 Jul 5. PMID: 35803296. ↩ ↩2
Hekkala A, Reunanen A, Koski M, Knip M, Veijola R, Finnish Pediatric Diabetes Register. Age-related differences in the frequency of ketoacidosis at diagnosis of type 1 diabetes in children and adolescents. Diabetes Care 2010; 33: 1500–2. ↩